Treating glue ear
Most cases of glue ear will clear up by themselves, but a temporary hearing loss as a result of a prolonged episode of glue ear can affect a child’s speech and language development and you may also notice a change in their behaviour.
Going to the doctor
You should take your child to see your GP who will examine your child’s ears and see if they have glue ear. Your GP may monitor your child to see if the glue ear resolves by itself. If it doesn’t, your GP will refer your child to the audiology or ear, nose and throat (ENT) department at your local hospital for a hearing test.
If your child is diagnosed with glue ear and their hearing is affected, the audiology or ENT department at the hospital will monitor the glue ear over a period of three months. This is known as ‘watchful waiting’. At the end of this period, your child’s hearing will be retested to see if the glue ear has resolved.
If there’s no improvement, surgical intervention, such as grommets, or hearing aids may be offered.
Grommets
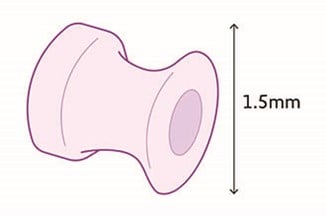
Grommets are tiny plastic tubes that are put in the eardrum. They allow air to circulate in the middle ear and help to reduce the fluid from further building up. This is usually done as a day case and is a short operation in hospital under general anaesthetic. The grommets are inserted after the fluid in the middle ear has been drained away.
A discharge (occasionally blood-stained) may occur for a couple of days immediately after the operation. After this time there shouldn’t be any discharge. If there is, you should see your GP for advice and antibiotic drops. Any prolonged discharge from the ear should be assessed by your ear, nose and throat (ENT) doctor.
Grommets usually stay in for around 6–12 months until the eardrum has healed and pushed them out. Sometimes the fluid comes back and another grommet operation may be considered.
See tips about preparing your child for surgery.
Our comic for children under 10, Harvey Gets Grommets, explains why Harvey gets grommets, what happens when he visits the doctor, and what happens at the hospital when the grommets are put in.
Swimming and bathing with grommets
Your ENT doctor will recommend keeping your child’s ears dry for the first 2–4 weeks immediately following the surgery. After this, most children with grommets don't need to take any special precautions and can swim and bath as usual with grommets in. There are a few children who may be at a particular risk of infection due to water entering the ear. If your child is one of these, your ENT doctor may suggest some of the following precautions.
- Try to avoid your child diving or jumping into the water as this increases the outside pressure and forces water through the grommet into the middle ear.
- Use earplugs and neoprene headbands, such as the Ear Band-It.
- Try to get your child to wear a swimming cap.
- Avoid your child swimming in lakes or non-chlorinated pools. The water in these places usually has a high bacteria count and infection is more likely to occur.
- Be careful when washing your child’s hair. Soapy water is able to slip more easily through the grommet into the middle ear. If the water is dirty it will infect it. With your child sitting upright in the bath, wash their hair first before body washing. Tilt their head back and rinse with clean water, then apply a shower cap. This way your child can play in the bath without getting dirty, soapy water in their ears.
Otovent nasal balloon
The Otovent nasal balloon (also known as nasal balloon autoinflation) is a non-surgical, drug-free treatment option for glue ear. Autoinflation is a method of encouraging the eustachian tube to open. This can help drain the ear naturally through the eustachian tube, by forcing air from the back of the throat to the middle ear.
The Otovent is suitable for children from three years old. It consists of a balloon and a nosepiece. This treatment involves fitting the balloon to the nosepiece, putting the nosepiece against one nostril and keeping the other nostril and mouth closed. By blowing through the nostril, the balloon is inflated until it’s about the size of a grapefruit. The nosepiece is removed and the procedure repeated with the other nostril.
The Otovent may be helpful for some older children during the watchful waiting period or while waiting for grommet surgery.
Otovents are available on prescription. Ask your GP or ENT consultant about whether they think it will be suitable for your child.
You can also watch the demonstration video produced by the University of Southampton or find out more information from the Otovent Glue Ear Treatment video.
Hearing aids
Hearing aids are devices designed to make sounds louder. They are used on a temporary basis for glue ear while waiting either for the glue ear to resolve or for grommet surgery. For children who have repeated problems with glue ear or are unable to have grommet surgery, hearing aids can be very helpful.
Good quality, digital hearing aids are available free of charge for all children on the NHS. Your child may also be offered a bone conduction hearing device.
Read about Cody who still has glue ear at the age of 12.
Alternative treatments for glue ear
In 2023, the National Institute for Health and Clinical Excellence (NICE) published guidance about glue ear for the NHS in England and Wales. Having studied all the research evidence available, they made recommendations on the use of various treatments for glue ear based on which treatments effectively treated the greatest number of children. NICE currently recommends grommets or hearing aids as effective treatments for glue ear.
At the current time NICE does not recommend using:
- steroids
- antihistamines
- decongestants
- antibiotics
- homeopathy
- cranial osteopathy
- acupuncture
- massage
- probiotics
- changing the diet (for example, to reduce dairy)
- immunostimulants.
For some treatments, there may be very little or poor quality evidence available. Some may also be offered by the alternative or complementary health sector, which does not tend to produce the type of scientific evidence reviewed by NICE.
How we can help
We are here for all children and young people who are deaf or experience temporary hearing loss, including glue ear.
Join us for free to get access to one-to-one guidance from our experts, the chance to meet other families of deaf children and children experiencing glue ear, plus regular updates on the topics that are most important to you.
My daughter and glue ear
Parents Peter and Rachel discuss the treatment options for glue ear they chose for their daughter, Libby, and how we helped them make the right decisions for their family.